
I will be honest, I was really surprised that his bilirubin levels didn't go down quickly, after he started drinking the water. I think I was getting bilirubin confused with ammonia. The water machine makes water tha it myself.t is known to reduce ammonia levels. I saw a doctor on a video say that it lowers it, and I've seen this happen with many people who've gotten water machines. So, I couldn't help thinking, what is going on, here?? Why won't this guy's bilirubin levels come down??
Well, as you can see in my previous post, I learned that furosemide can elevate bilirubin levels (or at least, this makes it harder for the body to process and eliminate it). This guy I was trying to help, was very bloated due to the fact that the doctors felt that they could not do a paracentesis on him. They felt that he was at too high of a risk for bleeding. So they kept giving him furosemide, and this makes a person's bilirubin levels go up!!!
PLEASE SEE MY ORIGINAL POST ABOUT BILIRUBIN, BLUE LIGHTS, AND HOW FUROSEMIDE CAN INCREASE BILIRUBIN, BY CLICKING HERE.
On Monday evening, I was trying to find a place where Lisa could get blue lights to help her son reduce his bilirubin. I am about an hour and 15 minute drive from where her son is, at the hospital. I had a lot of work to do that evening, but I knew she was overwhelmed and busy and probably didn't want to leave the hospital because her son was so sick. So, I made some calls to see where she might be able to pick up blue lights. I called an aquarium store but they didn't have much in terms of blue light (just one that was kind of half blue, half white... which, who knows, might be even better but I'm just going for all-blue since that's what we know is given to jaundiced babies).
What I would REALLY like to be able to post a link for, is the BILIBLANKET. But these are not readily available to people... at least, you can't just go order one straight off amazon. You have to fill out a form.... just like I have to make people fill out a form, for the water, because it's medical equipment and you need to to talk to someone who can make sure you'll know how to use it. There's an interesting discussion on this page, where you can see the biliblanket really does seem to help lower bilirubin levels. But you'll see in the comments section, one person says sunlight works BETTER than a blue light. And I would NOT be surprised if this is true!! I found it a bit suspicious and odd that this guy I was trying to help, was in the hospital for weeks, and the doctors and nurses easily could have put his bed by the window... but they did not!
https://thehappyhospitalist.blogspot.com/2011/04/how-fast-does-biliblanket-work-not-fast.html
I called the Home Depot in her area (hoping she could have her daughter go pick them up) and I am not kidding, I was on the phone, on hold, for OVER AN HOUR, trying to reach someone who could tell me if they had blue lights. When I finally DID get ahold of someone, I was told that no, they don't seem to have the blue lights I was looking ofr. So lame.

 I went into an Ace hardware store in my neighborhood, and saw these lights, which do not look like they would have the ability to "turn blue" because the glass part doesn't look blue at all.... but boy, did they ever emit some blue light!
I went into an Ace hardware store in my neighborhood, and saw these lights, which do not look like they would have the ability to "turn blue" because the glass part doesn't look blue at all.... but boy, did they ever emit some blue light! 

 The kid who works there is always super helpful, and he did some research on the store's computer to see if these are supposed to emit blue light... and sure enough.... they really do. I was looking for a wavelength in around the 450 nm range, because that's what's used for babies with jaundice in hospitals. Apparently, it seems that blue light in general is kind of the same across the board, in terms of the wavelength it delivers. He turned it on for me and I went WHOAH! Now that is some seriously strong blue light!!!
The kid who works there is always super helpful, and he did some research on the store's computer to see if these are supposed to emit blue light... and sure enough.... they really do. I was looking for a wavelength in around the 450 nm range, because that's what's used for babies with jaundice in hospitals. Apparently, it seems that blue light in general is kind of the same across the board, in terms of the wavelength it delivers. He turned it on for me and I went WHOAH! Now that is some seriously strong blue light!!!


Stuff I bought this stuff from the hardware store...

I set them up at home, using some microphone stands and duct tape. They looked good, and really bright. So, I called Lisa and said look, if you would like to use these, I will drive them to you. I got a friend to drive me (the check engine light has been coming on, on my car, so I was wary of driving my own car at night!)

 Bringing the mic stands to the room, in the elevator... being held by a good friend who has the perfect commuter van (that we weren't worried about breaking down on the freeway : D).
Bringing the mic stands to the room, in the elevator... being held by a good friend who has the perfect commuter van (that we weren't worried about breaking down on the freeway : D).
This is how it looked, when we set it up above the hospital bed.

The other thing I don't like, is that a person has to expose their skin to the light, and the hospital rooms can be cold. In my opinion, it's far better to use something that you could keep UNDER a blanket. Once again.... it is soo frustrating to me, that you can't just order a biliblanket on amazon. I don't get it. I even looked on Alibaba to see if maybe they sold something like that, but... no dice. I know I probably COULD order a biliblanket, but.... it just sounded like a hassle.
Well, I know this may sound a little nuts, but if it really is true that regular blue LED lights, like christmas tree lights, emit the same frequency as a large blue light, or a bilirubin blanket light... then wouldn't you be able to use a rope light, under a blanket, like this?
CLICK HERE (or on the pic) to see these rope lights on Amazon. They're UL approved, and have really good reviews! If I had a relative, I'd stitch these lights into a blanket and have them sleep with it at night. By the way, the big blue lights I bought from the hardware store were cool to the touch, so I'm not too concerned about something like this catching fire. I guess you have to weigh the odds of everything, and in my opinion, the odds of dying from extremely high bilirubin the doctors can't get down are 50-50. The odds of dying from a blanket catching fire are maybe one in a million. So I'd go with the lights!
CLICK HERE to see the rope lights (click on the pic for the blue ones when you're on the page).

I bought a bunch of these blankets from Costco and they are SOOOO cozy. They ran out, but you can still get them online from Amazon.

Bedsure Sherpa Throw Blanket Navy Blue 50"x60" Reversible Fuzzy Bed Throws Microfiber All Seasons Luxury Fluffy Blanket for Bed or Couch by
One thing I am trying to understand is, how it is that bilirubin is considered highly toxic, and yet, it is also an antioxidant.... in both forms - conjugated and unconjugated.
It appears that the blue lights do a good job of turning the bilirubin into the conjugated form, so it can be excreted in urine and feces.
I posted lots of articles and web pages I had scoured through, trying to figure out how to help this poor guy solve the bilirubin problem (sometimes I think of this blog as a big scrapbook where I can save articles and links for my own reference, and share it with others at the same time). I still don't have the answers, but feel like I am getting closer. I also want to do some more research on natural light and jaundice.
UPDATE: Oh... my.... God. OK so I just did a quick google search on this, and.... sure enough.... babies that were treated with NATURAL SUNLIGHT had a greater improvement, than babies that were treated with artificial sunlight!!!! So why they would keep this poor guy in a hospital bed AWAY FROM THE WINDOW is beyond me.... well, no... sadly, it's not beyond me. It makes perfect sense to me. As long as he didn't get better, then could charge him for another two weeks of hospitalizations.
You can see the article I read, here:
https://www.nytimes.com/2015/10/20/health/filtered-sunlight-is-good-cure-for-infant-jaundice-study-says.html
And I will copy and paste it at the bottom of this post, in case the link breaks or the article disappears.
Filtered sunlight is a cheap, effective way to treat infant jaundice, according to a study by Stanford researchers.
Jaundice — caused by an excess of bilirubin in the blood — leads to brain damage or death in about 150,000 babies a year in poor countries. The problem is common in newborns, whose livers sometimes need several days after birth to generate the enzymes needed to break down bilirubin, which is released when red blood cells break down. Yellow skin and eyeballs are common symptoms.
In wealthy countries, jaundiced newborns are placed for several days under sunlamps that emit extra blue wavelengths of light and minimal ultraviolet or infrared ones.
It was established during World War II that artificial sunlight cures jaundice, which more than 28,000 soldiers developed after getting yellow fever vaccine made from human blood.
For years, American research focused on drugs to block bilirubin formation, while hospitals relied on lamps and, in extreme cases, transfusions to treat patients.
But hospitals in poor countries may be unable to afford lamps or may lack a steady electricity supply to run them.
The Stanford team, whose workwas published last month in The New England Journal of Medicine, tested whether real sunlight —which is plentiful at many hospitals in tropical climes — could be made safe enough for babies to lie in for hours a day.
They treated 433 babies for jaundice at a hospital in Lagos, Nigeria. Half received sunlamp phototherapy, and half slept in outdoor cribs or their mothers’ laps under canopies of plastic film that filtered out ultraviolet and infrared rays.
The sunlight treatment was slightly more effective, and the children did not have more sunburn, dehydration or overheating.
The researchers have designed a small greenhouse to be used in windier or colder climates.
https://www.ncbi.nlm.nih.gov/pubmed/11001835
Mol Genet Metab. 2000 Sep-Oct;71(1-2):411-7.
Bilirubin oxidation in brain.
Abstract
Bilirubin is a product of heme catabolism which by virtue of its lipid solubility can cross the blood-brain barrier and enter the brain. Neonatal jaundice is a common transitional phenomenon which is due to the combination of increased heme catabolism and rate limitations as far as hepatic conjugation and biliary excretion of bilirubin. In the great majority of cases this is an innocuous condition, which is even posited to have some beneficial effects due to the ability of bilirubin to quench free oxygen radicals. However, because bilirubin is neurotoxic, hyperbilirubinemia in the newborn may exceptionally result in death in the neonatal period, or survival with severe neurological sequelae (kernicterus). Bilirubin enters the brain through an intact blood-brain barrier. Clearance of bilirubin from brain partly involves retro-transfer through the blood-brain barrier, and possibly also through the brain-CSF barrier into CSF. Work in our lab during the past 5 years has substantiated earlier work which had suggested that bilirubin may also be metabolized in brain. The responsible enzyme is found on the inner mitochondrial membrane, and oxidizes bilirubin at a rate of 100-300 pmol bilirubin/mg protein/minute. The enzyme activity is lower in the newborn compared with the mature animal, and is also lower in neurons compared with glia. Studies of different rat strains have documented genetic variability. The enzyme is cytochrome-c-dependent, but has as yet not been unequivocally identified. The rate of oxidation of bilirubin is such that this enzyme probably contributes meaningfully to the clearance of bilirubin from brain.
Background
Jaundice refers to the yellow appearance of the skin that occurs with the deposition of bilirubin in the dermal and subcutaneous tissue. Normally in the body, bilirubin is processed through the liver, where it is conjugated to glucuronic acid by the enzyme uridine diphosphate glucuronyl transferase (UGT) 1A1. This conjugated form of bilirubin is then excreted into the bile and removed from the body via the gut. When this excretion process is low following birth, does not work efficiently, or is overwhelmed by the amount of endogenously produced bilirubin, the amount of bilirubin in the body increases, resulting in hyperbilirubinemia and jaundice.
Jaundice occurs in as many as 60% of all normal newborns within the first week of life. [1] Jaundice in the newborn can occur from an underlying pathological condition, such as isoimmune hemolysis or an RBC enzyme deficiency
https://www.ncbi.nlm.nih.gov/pubmed/4019432
https://www.ncbi.nlm.nih.gov/pubmed/2768223
https://www.ncbi.nlm.nih.gov/pubmed/8486217
Articles looked at:
https://en.wikipedia.org/wiki/Glucuronic_acid
https://www.ncbi.nlm.nih.gov/pubmed/4019432
https://www.ncbi.nlm.nih.gov/pubmed/2768223
https://www.google.com/search?q=drug+that+causes+contact+lenses+to+turn+pink&rlz=1C1CHBF_enUS696US696&oq=drug+that+&aqs=chrome.0.69i59j69i57j0l4.10806j0j7&sourceid=chrome&ie=UTF-8
https://www.ncbi.nlm.nih.gov/pubmed/4019432
https://www.ncbi.nlm.nih.gov/pubmed/2768223
J Biochem. 1989 Jun;105(6):968-73.
Protection of glutathione S-transferase from bilirubin inhibition.
Abstract
Inhibition of the enzyme activity of glutathione S-transferase (GST) by a physiological concentration of bilirubin was studied using various substrates. When rat liver cytosol was used as an unfractionated GST, its GSH-conjugation activity toward 1-chloro-2,4-dinitrobenzene was decreased to one-half by bilirubin, while the activity toward 1,2-dichloro-4-nitrobenzene, p-nitrobenzyl chloride, or 1,2-epoxy-(p-nitrophenoxy)propane and also the non-selenium dependent GSH-peroxidase activity toward cumene hydroperoxide (CHPx activity) were hardly affected under the same conditions. In contrast, bilirubin inhibited each of the purified GST isozymes and no remarkable difference in bilirubin inhibition was observed with any of the substrates tested. From the chromatographic analysis of the cytosol incubated with [3H]bilirubin, it was found that a major part of the added bilirubin binds to subunit 1 (Ya) of GST isozyme, leaving not only the conjugation activity derived from 3-4 type GST but also the CHPx activity of subunit 2 (Yc) quantitatively intact. The bilirubin inhibition of both the conjugation activity of GST 3-4 and the CHPx activity of GST 2-2 was prevented almost completely by addition of a 3-fold molar excess of GST 1-1. From these results, it was assumed that the enzyme activities of both 3-4 type GSTs and subunit 2 (Yc) were protected from the inhibitory action of bilirubin by the scavenger effect of subunit 1 (Ya).
- PMID:
- 2768223
https://www.ncbi.nlm.nih.gov/pubmed/8486217
Relationship between biliary excretion of bilirubin and glutathione disulfide.
Abstract
The effects of two glutathione-oxidizing agents, t-butyl hydroperoxide and diamide, on biliary excretion of bilirubin and glutathione disulfide were investigated in anesthetized male Sprague-Dawley rats. Bilirubin (unconjugated) was infused at a constant rate of 100 nmol/kg/min through the jugular vein. When biliary excretion of bilirubin was stabilized, either of the glutathione-oxidizing agents was administered via the mesenteric vein. Biliary excretion of glutathione disulfide increased temporarily after the administration and returned to its basal levels within 20 min. The biliary excretion of bilirubin decreased during the same period and returned to the former levels thereafter. Changes in bile flow rates remained within 20% of the basal levels. A linear correlation was found between the increments in the bile concentration of glutathione disulfide and the decrements in that of bilirubin. Furthermore, separate experiments revealed that reduction of hepatocellular glutathione per se had little effect on biliary excretion of bilirubin. The results thus indicate that the reduction of biliary excretion of bilirubin by glutathione-oxidizing agents was due to the increase in biliary excretion of glutathione disulfide, and suggest that a common biliary excretory mechanism is shared, at least partially, by bilirubin and glutathione disulfide in Sprague-Dawley rats.
- PMID:
- 8486217
Articles looked at:
https://en.wikipedia.org/wiki/Glucuronic_acid
https://www.ncbi.nlm.nih.gov/pubmed/4019432
https://www.ncbi.nlm.nih.gov/pubmed/2768223
https://www.google.com/search?q=drug+that+causes+contact+lenses+to+turn+pink&rlz=1C1CHBF_enUS696US696&oq=drug+that+&aqs=chrome.0.69i59j69i57j0l4.10806j0j7&sourceid=chrome&ie=UTF-8
Rifadin (rifampin) Drug Side Effects, Interactions, and Medication ...
https://www.emedicinehealth.com/drug-rifampin/article_em.htm
Jump to What is the most important information I should know about rifampin ... - Before taking rifampin, tell your doctor if you are allergic to any drugs, or if you have liver disease or porphyria ( (a genetic enzyme disorder that ... This medicine may discolor your tears, which could permanently stain softcontact lenses.Fundamentals of phototherapy for neonatal jaundice.
Erratum in
- Adv Neonatal Care. 2007 Apr;7(2):65.
Abstract
Phototherapy is the use of visible light for the treatment of hyperbilirubinemia in the newborn. This relatively common therapy lowers the serum bilirubin level by transforming bilirubin into water-soluble isomers that can be eliminated without conjugation in the liver. The dose of phototherapy largely determines how quickly it works; the dose, in turn, is determined by the wavelength of the light, the intensity of the light (irradiance), the distance between the light and the infant, and the body surface area exposed to the light. Commercially available phototherapy systems include those that deliver light via fluorescent bulbs, halogen quartz lamps, light-emitting diodes, and fiberoptic mattresses. Proper nursing care enhances the effectiveness of phototherapy and minimizes complications. Caregiver responsibilities include ensuring effective irradiance delivery, maximizing skin exposure, providing eye protection and eye care, carefully monitoring thermoregulation, maintaining adequate hydration, promoting elimination, and supporting parent-infant interaction.
- PMID:
- 17208161
- DOI:
- 10.1016/j.adnc.2006.08.004
- [Indexed for MEDLINE]
https://www.ncbi.nlm.nih.gov/pubmed/17208161
https://profreg.medscape.com/px/registration_ab.do?lang=en&src=ban_acq_1707_mscpmrk_728x90_ref
http://www.meddean.luc.edu/lumen/meded/orfpath/bilirub.htm
Ask the Diet Doctor: The Deal with Detoxifying Foods
https://www.shape.com/blogs/ask-diet-doctor-deal-detoxifying-foods
1. Calcium D-glucarate. Your liver functions as both your metabolic brain and filter. It identifies compounds such as hormones, environmental toxins, or carcinogens that should not be present (or should not be present at high levels) and sends these compounds down the pathway for excretion from your body (a.k.a. detoxification). One of the ways that your body flags these toxic compounds for removal is by binding them to glucuronic acid. Unfortunately your body also contains an enzyme, beta-glucuronidase, that removes glucoronic acid from toxins flagged for removal. This is where calcium D-glucarate, or glucaric acid, from broccoli comes in. Glucaric acid inhibits beta-glucuronidase from working so when your liver flags a toxin for removal, beta-glucuronidase cannot undo this action. The end result is that more toxins get excreted faster.
One of the ways that your body flags these toxic compounds for removal is by binding them to glucuronic acid. Unfortunately your body also contains an enzyme, beta-glucuronidase, that removes glucoronic acid from toxins flagged for removal. This is where calcium D-glucarate, or glucaric acid, from broccoli comes in.
Glucuronidation is a process by which a glucuronide group is added to a molecule and signals for said molecule to be excreted via the kidneys (urinated). D-Glucaric acid, via its metabolite, inhibits the removal of the glucuronide group and preserves/promotes excretion of any molecule that is subject to glucuronidation
Endogenous substances that are known to be glucuronidated (and thus can potentially have their excretion enhanced by D-glucaric acid supplementation) include steroid hormones,[7] and bilirubin.
Size: 90 Count - Old LabelChange
Price:$60.11+ Free shipping
Summary of Calcium-D-Glucarate
Primary Information, Benefits, Effects, and Important Facts
For the most part, Calcium-D-Glucarate is just known to be a β-glucuronidase inhibitor via its metabolite D-glucaro-1,4-lactone. The process of 'glucuronidation' is a detoxification process where a group (known as a glucuronide) is attached to a hydrophobic molecule to make it more water soluble, and then the kidneys can better facilitate its removal from the body. This process is positively mediated by the glucuronosyltransferase enzyme, and negatively mediated by the β-glucuronidase enzyme; as such, inhibiting the negative regulator (the enzyme that removes the glucuronide) indirectly increases the activity of this pathway.
It is touted to be an anticancer agent, which is due to a series of past research done in rats and mice exposed to the DMBA toxin which is known to be glucuronidated. There are definitely anticancer effects in these models, and it appears to extend to other toxins that are glucuronidated.
However, a problem occurs when humans take this as an oral supplement. Although it appears to be safe even at high doses, very high doses are required for its effects (100mg/kg minimum, near maximal effects at 200mg/kg) and this would even only theoretically assure some protection against toxins that are glucuronidated. If a toxin is subject to another detoxification pathway (such as conjugation by glutathione) then Glucaric acid will serve no benefit.
Organ cancer production which just occurs spontaneously because of oxidative stress to DNA is also not likely to be protected against, as increasing glucuronidation does not per se decrease oxidative stress in the body (it might just reduce the oxidative effects of toxins).
Furthermore, all steroid hormones in the body (testosterone, estrogen, DHEA, etc.) are also glucuronidated. If using an oral dose that reduces the toxin, these hormones will also all be reduced for a short time.
Using calcium-D-glucarate as a daily preventative supplement does not appear to be a prudent idea, due to its lack of reliability even in theory and high doses used. However, a single acute dose of this supplement prior to known exposure to toxins that are glucuronidated (such as both benzopyrene and polyaromatic hydrocarbon compounds produced in the cooking of meat products) might be more prudent and potentially useful.
| Price: | $60.11 ($0.67 / Count) & FREE Shipping |
Note: Not eligible for Amazon Prime.
Only 15 left in stock - order soon. Ships from and sold by eHerbal USA.
Get it as soon as April 23 - 26 when you choose Economy Shippingat checkout.
3 new from $60.11
Other Sellers on Amazon
| Made by Amazon, Tested for Purity |
 Melatonin 3mg $9.99 |  Men's Multivitamin $21.99 |  Biotin $10.39 |  Turmeric Complex $16.99 |
Thorne Research - Calcium D-Glucarate - To Enhance Liver Detoxification - 90 Capsules







J Gastroenterol Hepatol. 2013 Jul;28(7):1202-8. doi: 10.1111/jgh.12155.
Unconjugated bilirubin, a potent endogenous antioxidant, is decreased in patients with non-alcoholic steatohepatitis and advanced fibrosis.
Abstract
BACKGROUND AND AIM:
Oxidative stress is considered a key element in the progression of non-alcoholic fatty liver to non-alcoholic steatohepatitis (NASH). Unconjugated bilirubin is the main endogenous lipid antioxidant and is cytoprotective in different tissues and organs. In this study, it was evaluated if unconjugated bilirubin levels are associated with the degree of liver injury in patients with non-alcoholic fatty liver disease.
METHODS:
Two hundred and eighty-five patients were retrospectively evaluated with biopsy-confirmed non-alcoholic fatty liver disease. Multiple logistic regression models were used to assess the relationship of steatosis, inflammation, and fibrosis levels to the features of patients.
RESULTS:
Unconjugated bilirubin levels differed significantly according to inflammation and fibrosis scores. Unconjugated bilirubin was lower in patients with moderate-severe inflammation compared with those with absent-mild (P = 0.001) and in patients with moderate-severe fibrosis compared with those with absent-mild (P < 0.001), whereas no difference was observed for steatosis grades. At logistic regression analysis, low unconjugated bilirubin levels were associated with moderate-severe inflammation (odds ratio, 0.11; 95% confidence interval 0.02-0.76; P = 0.025) and moderate-severe fibrosis (odds ratio, 0.013; 95% confidence interval 0.001-0.253; P = 0.004).
CONCLUSIONS:
Low unconjugated bilirubin levels are independent predictors of advanced inflammation and fibrosis in patients with steatohepatitis, indicating the lack of antioxidant protection as a possible molecular determinant for the progression of liver injury.
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty Ltd.
https://profreg.medscape.com/px/registration_ab.do?lang=en&src=ban_acq_1707_mscpmrk_728x90_ref
http://www.meddean.luc.edu/lumen/meded/orfpath/bilirub.htm
li-11-1 BILIRUBIN METABOLISM By Dr. E. Orfei
Physiology and pathology
1-Bilirubin production.
2-Transport in blood.
3-Hepatocellular uptake.
4-Intracellular transport in hepatocytes.
5-Conjugation with glucuronic acid.
6-Secretion into bile ducts.
7- Intestinal metabolism.
8- Renal excretion of bilirubin
9- Renal excretion oh urobilinogen
1-BILIRUBIN PRODUCTION
Bilirubin is the terminal product of heme metabolism. Heme is present in hemoglobin and in other oxidative compounds such as hepatic mitochondrial and microsomal cytochromes (P-450). Thus plasma bilirubin is part erythropoietic and part non-erythropoietic. Approximately, 85 % erythropoietic and 15% non-erythropoietic.
The erythropoietic fraction originates from two sources: the circulating normal aging red cells and the immature defective red cells of the bone marrow. The daily production of bilirubin is 250 to 350 mg.
Shunt bilirubin is called that portion that does not originate from senescent circulating red cells but originates from immature and defective red cells (7%) and from non- hemoglobin heme compounds, particularly from hepatic cytochromes and from myoglobin. These two fractions were discovered by labeling hemoglobin with a radioactive glycin, and observing that one fraction (78 %) of bilirubin is excreted in the feces in 120 days and another fraction is excreted in 10 days or less. The first was called late labeled bilirubin, the second was called early labeled bilirubin or shunt bilirubin. Shunt bilirubin may be markedly elevated in certain pathologic states: sideroblastic anemia, megaloblastic anemia, erythroleukemia, lead poisoning and a congenital disorder called "idiopathic dyserythropoietic jaundice". The patients affected by this condition do not have hemolysis. They have hyperbilirubinemia and jaundice. The hyprbilirubinemia is due to shunt bilirubin.
Bilirubin from erythropoietic heme is produced by monocytic macrophages, reticulo-endothelium, in every organ but especially in the spleen, liver and bone marrow in order of importance.. The bilirubin from non-erythropoietic hepatic heme is produced in the hepatocytes.
The tetrapyrrolic ring of heme is broken by an oxygenase at the alpha bridge, the bond between the two carbons opposite to the gamma bridge which is between the two carbons carrying the two propionic acids. The tetrapyrrolic molecule from a ring is transformed into a tetrapyrrolic chain without iron.
HEME + Heme oxygenase = OXY- HEME ( closed tetrapyrrolic ring with iron)
OXY- HEME + heme reductase = BILIVERDIN (open tetrapyrrolic ring without iron)
BILIVERDIN + biliverdin reductase = BILIRUBIN (unconjugated)
Pathology of bilirubin production
Hyprbilirubinimia with jaundice occurs in increased destruction of red blood cells namely: hemolysis. It occurs in 1)congenital disorders of red cells (sickle cells, thalassemia, spherocytosis), 2) immune hemolysis (erythroblastosis fetalis, 3) acquired diseases of red cells (dyserythropoiesis), etc.
In the adult, even a marked hemolysis does not produce significant increase of serum bilirubin if the hepatic bilirubin clearance is normal. In the newborn, however, a marked hemolysis will be catastrophic. At levels of 20mg/dl of serum bilirubin the infant will be deeply jaundiced and will develop kernicterus (Nuclear jaundice: a grave form of yellow staining and degeneration of intracranial gray matter especially of lenticular nucleus, ammon,s horn and subthalamic area).
Phototherapy is used for treatment of hyerbilirubinemia in neonates.
Bilirubin is a photoreceptor. The blue light transforms bilirubin into colorless products of oxidation which are excreted in the urine.
Synthetic porphyrins containing tin or zinc instead of iron cause decrease of bilirubin formation by competing for the heme oxygenase activity of macrophages. These compounds have been used in the treatment of hyperbilirubinemia in animals and humans (e.g. Gilberts syndrome) with limited success.
2-BILIRUBIN TRANSPORT IN BLOOD
Bilirubin is toxic to tissues, therefore, it is transported in the blood bound to albumin. Only a minute amount of free form is present in the blood.
Pathology of bilirubin transport in blood.
If the free fraction increases, bilirubin will invade and damage the tissues. It will cross the blood -brain barrier and cause kernicterus in the neonate. Free plasma bilirubin can increase in the fallowing pathologic conditions:
-1- overproduction.
-2- defective conjugation in the hepatocyte.
-3- presence of substances interfering with bilirubin-albumin binding: sulphonamides , long-chain fatty acids from breast milk, salycilates, contrast media, etc. These agents compete for albumin binding sites.
3-HEPATOCELLULAR UPTAKE OF BILIRUBIN.
Bilirubin is taken up by hepatocytes at their sinusoidal surface. The albumin-bilirubin bond is broken. Albumin remains in the plasma. The free molecule of bilirubin enters the hepatocyte.This uptake is very rapid.
Pathology of bilirubin uptake by hepatocytes.
The impairment of uptake will result in unconjugated hyperbilirubinemia.
Occurrence:
1) Male fern oil jaundice. This oil was used to treat tape worm. (Aspidium).
3) Jegzichte sheep.
4-INTRACELLULAR TRANSPORT OF BILIRUBIN IN HEPATOCYTES.
In the hepatocye bilirubin is bound to cytoplasmic proteins: ligandins and Z protein. Ligandins are a group of enzymes that represent 2% of cytosolic proteins. Z proteins bind fatty acids. The primary function of these proteins is that of avoiding the reflux of free bilirubin into the blood. Apparently, the time lapse between uptake of bilirubin and cojugation is relatively long.
Pathology of intracellular transport.
No hperbilirubinemia and jaundice is known due to deficiency of ligandins.
5-CONJUGATION WITH GLUCURONIC ACID
One way for cells to neutralize unwanted compounds is to conjugate them with a modified sugar, a glycosyl. The sugars used for this reaction are xylose, glucose or glucuronic acid. Glucose is normally present in the cell sap, xylose and glucuronic acid are formed from glucose by UDP-glucose dehydrogenase. Xylosidation is predominant in plants, glucosidation in bacteria and glucuronidation in mammals. Unconjugated bilirubinin is lipophilic. Its conjugation with glucuronic acid renders it hydrophilic, thus, it can be eliminated in the bile. Many other agents are eliminated by conjugation with glucuronic acid: steroids, thyroid hormone, catecholamines, estradiol, testosterone, bile acids, phenols, morphine, which can be conjugated by other cells besides hepatocytes.
The glucuronidation of bile proceeds in two steps: first glucuronic aid (GA) is synthesized from cytosolic glucose that is complexed with uridinediphosphate (UDP) ad forms udpglucuronic acid (UDPGA). From this compound, the glucuronic acid is transferred to blirubin. The first reaction is catalyzed by a UP- glucose dehydrogenate, the second reaction is catalyzed by bilirubin- DUGAN- transferees that is synthesized by microsomes. Any deficiency of these two enzymes will result in defective conjugation and elimination of bilirubin. On the other end, administration of microsomal enzyme inducers such as phenobarbital, glutethimide and antipyrine favor bilirubin conjugation and elimination by increasing blirubin transferase activity. Conjugation occurs in the endoplasmic reticulum and consists of forming an ester between glucuronic acid and one or both propionic side-chains of bilirubin. The result will be formation of bilirubin mono and di-glucuronides. In general, about 80% of the di and less than 20% of the mono are formed. Human bile cotains also small amounts of unconjugated bilirubin. In summary:
GLUCOSE + UDP-Glucose-dehydrogenase = UDP-GLUCURONIC ACID (UDPGA)
UDPGA + BILIRUBIN + Glucuronyl transferase = BILIRUBIN MONO &
DI- GLUCURONIDES.
Pathology of bilirubin conjugation
GILBERT�SYNDROME
Is due to a very mild deficiency of glucuronyl transferase.It is a very frequent disorder. It affects 5 to 7% of the general population. More common in males. It consists of mild fluctuating jaundice due to non- hemolytic unconjugated hyperbilirubinemia in the range of 5 to 7mg/dl or rarely higher. The liver is morphologically normal. State of health and life-span are normal. Hemolysis, low caloric diet, nicotinic acid will increase the jaundice. A lipid diet will decrease the jaundice. Phenobarbital and other enzyme inducing agents are beneficial. Some individuals with this syndrome beside a defect of bilirubin
CRYGLER-NAJJAR SYNDROME, TYPE I
Is due to a severe deficiency of glucuronyl tranferase. Deep jaundice develops tat birth, High serom unconjugated hyprbilirubinemia, >20 mg/dl., not responding to phenobarbital. Absent formation of diglucuronides. Death usually in the first year or two with kernicterus. Phototherapy, plasmaferesis and albumin exchange are beneficial. Liver transplantation may be life-saving. The liver is histologically normal. A similar condition exists in Gann rat. Fortunately this syndrome is rare. Only 100 or more cases have been described. It is apparently a hereditary autosomal recessive trait.
CRYGLER- NAJJAR SYNDROME TYPE II
Is due to a moderate deficiency of glucuronyl transferase. Milder unconjugated hyperbilirubinemia responding to enzyme inducing agents: phenobarbital, gltethimide, phenazone, chlorpromazine. Both, mono and di-glucuronides are formed. Patients develop normally but some may suffer bilirubin encephalopathy, kernicterus. They will have unremitting jaundice for the whole life. It is a familial disorder. The mode of genetic transmission is not clear.Thi defect of conjugation may have an associated defect of bilirubin uptake by hepatocytes.
PYSILOLOGICAL JAUNDICE OF THE NEWBORN.
It is due to a very transient insufficiency of glucuronyl transferase. During the first few days of life there is an overproduction of bilirubin and an underdeveloped mechanism of the liver to dispose of bilirubin.
Together with deficient conjugation, bilirubin production, blood transport, hepatic uptake and secretion are all deficient. Sometimes extrahepatic factors exist to aggravate the situation: infections, drugs competing for binding sites of bilirubin and above all, breast feeding. The long chains of fatty acids of the breast milk interfere with bilirubin-albumin binding sites.
6- BILE SECRETION FROM HEPATOCYTES
The liver is an endocrine and an exocrine gland. It secretes synthesized products internally into the blood through the sinusoidal surface such as blood proteins, coagulation factors etc. and secretes external into the biliary tract and the intestine bile and many other substances, the terminal products of detoxifying function. The mechanism of this external secretion is the least clear in the physiology of the liver. It seems that many cellular organelles are involved in this process: vesicles, Golgi complexes, lysosomes, plasma membranes, mitochondria, cytoskeleton, plasma membranes, canalicular villi. Are however clear the consequences of the malfunction of this apparatus especially in the secretion bile which will result in conjugated hyperbilirubinemia.
Pathology of bile secretion
DUBIN-JOHNSON SYNDROME.
The syndrome consists of chronic benign jaundice due to conjugated hyperbilirubinemia without pruritus or elevation of serum alkaline phosphatase nor histological evidence of cholestasis. The hepatocytes contain an abundance of coarse dark-brown pigment similar to melanin . The liver is black but normal. Serum bilirubin ranges between 2 and 20mg/dl, 60% conjugated. Jaundice appears in the first 3 decades of life and is intermittent. Sometimes the onset is acute, simulating a hepatitis. The prognosis is excellent. The disease is inherited as autosomal recessive trait. The diagnosis is made by needle biopsy. Corriedale sheep have similar black liver disease.
Click on the pictures to enlarge
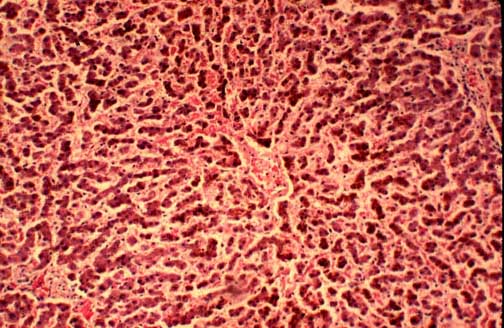 Fig.11-1-1 Dubin-Johnson Syndrome. Fig.11-1-1 Dubin-Johnson Syndrome.
The liver is brown-black because of the large amount of brownish coarse pigment stored in the hepatocytes. Typically there is no intrahepatic cholestasis in this condition. The pigment predominates in the centrolobular zone.
|
 Fig.11-1-2 Dubin-Johnson Syndrome. Fig.11-1-2 Dubin-Johnson Syndrome.
There could be a moderate portal fibrosis in older patients. The pigment is stored in lysosomes like lipofuscin. Bile canaliculi do not contain bile. According to studies conducted in Corriedale sheep, the pigment contains a melanin-like component and and its formation is attributable to a defect of excretion of epinephrine metabolites.
|
ROTOR SYNDROME.
This is a condition similar to Dubin-Johnson. There is intermittent jaundice with conjugated hyperbilirubinemia, similar clinical course, excellent prognosis but no pigment in the liver tissue.
BENIGN RECURRENT INTRAHEPATIC CHOLESTASIS.
A syndrome characterized by recurrent attacks of rather severe jaundice. The attacks start usually before puberty but they may start later. They are preceded by 2-4 weeks of pruritus malaise, anorexia followed by
increasing jaundice without pain or fever and lasting an average of 2-3 months during each attack. It may last from tow weeks to two years.
Nausea, vomiting , abdominal pain and skin rash occur in some cases. An affected individual may have up to 30 attacks during his life. Biochemically these patients have elevated serum bilirubin, 10 to 20 mg/dl, mostly conjugated, elevated alkaline phosphatase and bile acids. Alpa-glutamyl transferase (GGT) is elevated. Serum bile acids are elevated 2-30 folds. Transaminases are occasionally markedly elevated. These abnormalities and the clinical symptoms disappear completely in disease-free intervals. In the cholestatic phase there is acinar zone 3 cholestasis with bile plugs and mononuclear cell infiltration in the cholestatic area. In some cases there may be mild hepatocytic damage and portal mononuclear infiltrate. These changes do not produce any fibrosis or cirrhosis. Liver biopsies taken during clear intervals were normal. The disorder is rather rare and appears to be familial with autosomal recessive character.
FAMILIAL RECURRENT INTRAHEPATIC CHOLESTASIS OF PREGNANCY.
This disorder is clinically and biochemically similar to benign intrahepatic cholestasis. It occurs in the third trimester of pregnancy when the estrogen level is the highest and disappears postpartum. The affected subjects appear to belong to families with benign intrahepatic cholestasis trait. Gonadal steroid appear to ply a determining role in the cause of this syndrome. Histology of the liver shows centrolobular cholestasis similar to benign intrahepatic cholestasis. It is most frequent in Scandinavia (1/100), Bolivia and Chile (1/10).The disorder is safe for the mother but not for the fetus who will suffer premature births and stillbirths due to placental infarcts. The mothers have higher incidence of gallstones. Sometimes the disorder manifests itself only with presence of pruritus without jaundice. (Pruritus gravidarum). The patients are not severely ill as in fatty liver of pregnancy, hepatitis, obstructive jaundice.
DRUG- INDUCED INTRAHEPATIC CHOLESTASIS.
Many drugs produce cholestasis. The first cases reported were due to chlopromazine and synthetic steroids now out of market (Nilavar). Synthetic oral contraceptives are high in the list. They appeared to act on sensitivity base and affect only sensitive individuals. Many appear to impair the secretory function of the hepatocytes. And the list is increasing with the advent of new drugs. The liver in these cases may show
marked and fatal necrosis.
POST-OPERATIVE INTRAHEPATIC CHOLESTASIS
It is attributable to the combined effect of bilirubin overload deriving from blood transfusions and to defect of hepatocytic secretory function. Usually the jaundice appears in 1-2 postoperative days and disappears in one or two weeks, Hyperbilirubinemia is predominantly conjugated with rater normal alkaline
phosphatase and transaminases.
BACTERIAL INFECTIONS
It is a form of intrahepatic cholestasis. The hyperbilirubinemia is conjugated in all cases. Elevation of serum alkaline phosphatase in some cases. Hepatic histology without much hepatocellular damage.
Three types of morphological changes have been described:
1-canalicular cholestasis , the most common, mostly pericentral without hepatocellular damage.
2-ductular cholestasis, characterized by the presence of big bile thrombi in bile ductules and canals of Hering at the periphery of portal fields. No bile plugs in interlobular bile ducts.
3-Toxic shock syndrome due to infection with staphylococcus aureus producing Toxic Shock Syndrome Toxin-1 (TSST-1). This toxin was produced by this organism growing in polyacrylate tampons in menstruating women. The liver suffers inflammation of intrahepatic bile ducts and canaliculi.
with rupture of bile ducts and microvesicular steatosis. There is inflammatory reaction in portal fields with
neutrophils, eosinophils lymphocytes and monocytes. There is centrolobular cholestasis in 50% of cases.
7- INTESTINAL METABOLISM OF BILIRUBIN
Bilirubin in the intestine is reduced to urobilins according to the following cascade:
BILIRUBIN GLUCURONIDE + bacterial or intestinal beta-glucuronidase = FREE BILIRUBIN
FREE BILIRUBIN + bacterial dehydrogenase = UROBILINOGEN (colorless)
UROBILINOGEN + dehydrogenase = UROBILIN (orange-yellow).
The bulk of bilirubin, urobilinogen and urobilin is excreted in the feces. Small amounts of bilirubin and urobilinogen are reabsorbed by the intestine and return to the liver. The bilirubin is recunjugated in the liver and re-excreted in the feces. The reabsorbed urobilinogen is excreted in the urine, about 4 mg/ day and 0,1 to 1 mg in a random urine sample.
Pathology of biliary excretion into the intestine
COMPLETE BILIARY OBSTRUCTION.
The bile does not reach the intestine therefore the feces are acholic. There is conjugated hyperbilirubinemia and bilirubinuria. Urobilinogen is not formed in the intestine and there is no urobilinogen in the urine. because since the bile does not reach the intestine, urolinogen is not formed.
PARTIAL BILIARY OBSTRUCTION.
Less bile reaches the intestine. Urobilinogen is formed but in smaller amounts. There is less conjugated hyperbilirubinemia, absent bilirubinuria and small amounts of urobilinogen in the urine.
HEMOLYSIS.
Hemolysis causes unconjugated hyperbilirubinemia. There is no bilirubinuria because unconjugated bilirubin is not hydrophilic and cannot be excreted in the urine. There is increased urobilinogen in the urine because more bilrubin reaches the intestine and more urobilinogen is formed an reabsorbed.
8- RENAL EXCRETION OF BILIRUBIN
Only conjugated bilirubin (the direct fraction) is excreted in the urine when its level in the plasma is increased above normal. It not present in the urine of normal subjects and it is not eliminated in the urine in cases of unconjugated (the indirect fraction) hyperbilirubinemia, such as in cases of hemolysis.
Only the small fraction of non-protein bound bilirubin in the plasma passes in the urine. Some drugs and bile salts which compete for protein binding (salicylates, sofosoxazole) increase The theshold of elimination depends on the degree of protein binding which varies and its quantity in the urine does not have clinical relevance.
Conjugated bilirubin can be demonstrated in the proximal renal tubules.
9-RENAL EXCRETION OF UROBILINOGEN
Urobilinogen is formed by bacteria in the small intestine and in the colon.
It is then reabsorbed by the small intestine and the colon and re-xcreted by the by the liver into the intestine almost entirely. A very small amount is therefore excreted into the urine: 0-4 mg/day. This amount will increase when more urobilinogen is formed or when the liver is sick and unable to re-excrete it. This amount will decrease when its formation in the intestine is decreased such as in the case of complete bile duct obstruction when the bile cannot flow to the intestine where urobilinogen is formed by the specific bacteria. The urobilinogen formed by bacteria in the small intestine is re-absorbed better than that formed in the colon.
No comments:
Post a Comment